Accreditation updates from The Joint Commission, CMS
Takeaways
-
- Many OR managers said they were overdue for a survey by The Joint Commission because of the pandemic. The Joint Commission is said to be 3,000 surveys behind.
- More checklists are being used by surveyors, which are available in The Joint Commission’s Perspectives and EC News newsletters.
- New in 2022 were the workplace violence standards, including harassment that can occur in department structures either laterally or with hierarchy involved.
- The Joint Commission is seeking to eliminate standards they believe are unnecessary or do not correlate to the CMS Conditions of Participation, as well as to add new and revised standards to reduce healthcare disparities.
An important reason for accreditation from The Joint Commission is that it allows hospitals to bill Medicare and Medicaid, under what is called “deemed status,” says John Rosing, MHA, FACHE, executive vice president and principal at Patton Healthcare Consulting, an affiliate of HBS of Langhorne, Pennsylvania. Rosing spoke at the OR Manager Conference in 2022.

John Rosing, MHA, FACHE
Accreditation is voluntary, but if an organization is not accredited, it is instead subjected to surveys testing compliance with the Centers for Medicare and Medicaid Services (CMS) Conditions of Participation (CoP), performed by their state agency acting on behalf of CMS. Many CoP still read as they did in 1965, when the Medicare program was first introduced, and many others have been added or changed since. Updates for the CoP are announced by CMS via Quality, Safety, and Oversight memos and the periodically updated State Operating Manual.
The Joint Commission has more than 300 standards, based principally on CoP and organized by chapters, in its manual on which organizations are scored. It also has a 16-page monthly newsletter, called “Perspectives,” which often has new surveyable requirements published within it, and a robust website that includes Frequently Asked Questions and other resources. A hospital’s accreditation coordinator should be monitoring these materials to stay on top of what is changing.
Validation surveys
CMS monitors accreditation surveyors’ performance by having the state agency do a validation survey within 4 to 6 weeks after about 5% of The Joint Commission’s surveys. CMS performs these surveys to try and find things The Joint Commission did not find, which are called “disparities.” CMS reports these disparities to an oversight committee of Congress every year.
There is usually a 35% to 40% disparity rate, which means CMS finds 35% to 40% additional findings during their validation surveys. “CMS obviously wants accrediting organizations to be more rigorous and accurate with their work,” says Rosing.
In recent years, CMS has experimented with doing validation surveys at the same time as The Joint Commission is on-site. They call them “co-validation” surveys. Those were disrupted with the COVID-19 pandemic, and it is not clear what is happening with the co-validation surveys currently, he says.
Many OR managers in the conference workshop said they were overdue for a survey by The Joint Commission because of the COVID-19 pandemic, and most said they were expecting a survey imminently.
Currently, The Joint Commission is said to be 3,000 surveys behind, notes Rosing. Those include surveys for hospitals, other accredited organizations, and disease-specific surveys like stroke care or total joint replacement programs. “CMS is very much interested in having them catch up,” he says.
There is no specific order to them doing it; it is based on the availability of surveyors, an organization’s geography, and the COVID-19 infection rate in the community. “Be ready if you are due,” he says.
New for 2022
Following is an overview of new requirements and standards:
Vaccination requirements.
New for 2022 were the COVID-19 vaccine requirements by CMS, with penalties for not having a 100% vaccination rate. These rules are still in place.
Workplace violence standards.
Also new were the workplace violence standards, which began in January. These standards include:
• Annual risk analysis of the worksite, including violence risks; fix what you find (Environment of Care [EC].02.02.01)
• Leadership oversight (Leadership [LD].03.01.01)
• Designated multidisciplinary team
• Policies and procedures on prevention and response
• Process for reporting, analyzing, trending incidents (EC.04.01.01)
• Follow-up and support for victims and witnesses
• Staff trained on reporting and program (Human Resources [HR].01.05.03)
• Report up to the board.
“Hopefully, your hospital has taken on this charge,” says Rosing. “This includes lateral harassment that can occur in department structures either laterally or with hierarchy involved. It’s not just the patient who gets violent; it can also be your colleagues,” he says.
Changes in resuscitation standards.
Changes in resuscitation standards that should have been put in place in 2021 and became effective January 2022 include:
• Reviewing regional variations in outcomes
• Encouraging evidence-based guidelines, staff training, data collection, and case review
• Creating new protocols for post-cardiac arrest care to reduce systemic effects of ischemia-reperfusion injury (Provision of Care [PC].02.01.20)
• Developing protocols based on scientific literature regarding assessment of neurological prognosis for patients who remain comatose after cardiac arrest (using multiple methods, as necessary)
• Following protocols for patient transfer to specialty care sites for post-cardiac arrest care
• Collecting data on resuscitation, outcomes, transfers (Performance Improvement [PI].01.01.01)
• Reviewing cases and data to improve program (PI.03.01.01).
Water management standards.
Water management is also new and something engineering staff are looking at to combat legionella, mainly, but other water-borne pathogens as well. Included in these standards are:
• Assign a team
• Have a system diagram (map water supply sources, treatment systems, processing steps, control measures, and end use points)
• Have a risk management plan based on the diagram
• Have mitigation plans for each step in the system
• Document monitoring and corrective actions
• Have an annual review (EC 02.05.02, Element of Performance [EP] 1-4)
• Reference American Society of Heating, Refrigerating and Air-Conditioning Engineers and Centers for Disease Control and Prevention documents.
Survey focus in 2022
The following are what the surveyor teams began focusing on in 2022:
• Surveyors start with evaluations in four key areas, referred to as 4-1-1: Suicide assessment, dialysis, sterile compounding, and high-level disinfection (HLD) and sterilization
• Screening process for COVID-19
• Sleep Lab equipment reprocessing
• EC and Life Safety (LS) standards: Air pressure relationships (eg, ORs positive, decontamination areas negative) electrical panels, eye washes, fire drills in offsite locations, exhaust hoods labeled as biohazard, kitchen Ansul (fire suppression system) activation
• Human Resources (HR) standards: Competencies, contracts, grievances
• Medications: Titratable medications and following orders for pain medications—“Following physician orders for titratable and pain medications have become a frequent finding,” says Rosing. “The surveyor studies the medical record, reviews the details of the order, and then compares the order to what the nurse administering the medication has documented in the Electronic Medication Administration Record. The nurse may chart an adjustment to the titratable medication rate or dose to properly care for a patient at that moment, but if that rate or dose is different than what was specified in the order, a finding results.”
• Assessments: Patient plan of care not matching the patient’s problem list or reason for admission
• Consents: “The main problem with consents is that they are not dated, timed, or signed by the provider or the person who gave the patient the information,” he says. “Another problem is that the consent is signed by the provider before actually meeting with the patient to share risk and benefit information and obtain consent. The electronic record is what trips providers up in this case. It automatically dates and time stamps any entries, and it will show if the physician, for instance, signed it the day before the procedure happened and before seeing the patient.”
• Documentation: History and physical, post-procedure notes, pre- and postoperative anesthesia assessment.
New surveying style
More checklists are being used by surveyors, and these checklists are available in The Joint Commission’s Perspectives and EC News newsletters. Organizations should get copies and inspect them themselves in advance, says Rosing. “It is somewhat of an open-book test because these checklists include essentially what the surveyors are going to ask you,” he says.
There is a survey activity guide that the organization’s survey coordinator should obtain and use. It goes through the objectives of the survey and each session or tracer, who should be involved, and how to participate.
Condition level findings are on the rise. “A condition level finding is one that rolls up into the condition category because of the risk or prevalence of the deficiency,” says Rosing. Condition level findings must be fixed as soon as possible because a surveyor will arrive within 45 calendar days to verify that a corrective action is in effect. “If you have condition level findings after a survey, you have to jump on your action plan and make sure it’s working by the time they come back and survey you again,” he says.
Survey schedule changes
Several changes have been put in place for surveys because of COVID-19 to avoid big meeting rooms of people gathered together.
Most notably, there will be a combination of sessions:
• This can be the lead surveyor’s decision.
• Medication Management (MM), IC, and Data Use are often planned to become combined sessions.
• Emergency Management (EM) has been separated back out from the Leadership (LD) opening session.
• Additional time has been provided for tracers: The tracer methodology is a key part of The Joint Commission’s on-site accreditation and certification survey process. It uses information from an organization to follow the experience of care, treatment, or services for a number of patients throughout the organization’s healthcare delivery process.
• There is more use of video meeting technology for team meetings. For example, an MM tracer used to be held in a conference room with 30 or more people. Now, it might be five in the room and 25 connected via a video meeting link.
• The opening conference will be conducted in a similar way. “There are going to be less people involved in person, and they will focus on the COVID-19 actions you have taken and what the current state of COVID is in your community,” says Rosing.
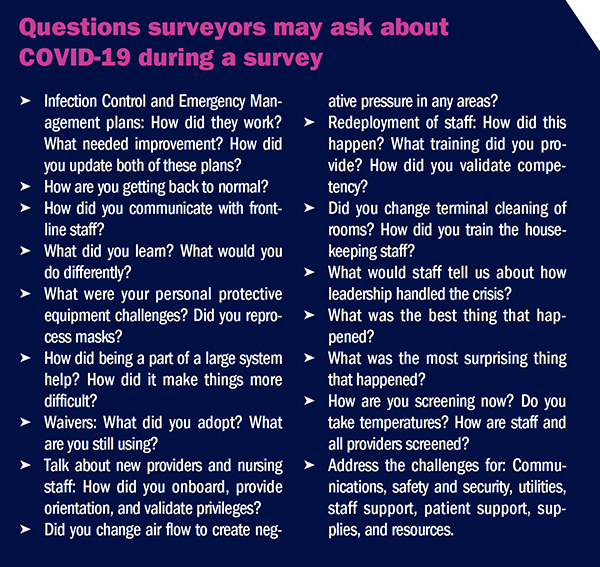
• Surveyors will have a list of questions to ask about COVID and how they were addressed (sidebar, Questions surveyors may ask about COVID-19 during a survey). “These are just questions to get surveyors familiar with your current status in the pandemic,” he says. “Your leadership will also be asked to describe what went on during the full course of the pandemic.”
Scoring for immediate threat to health and safety
Similar to the CMS immediate jeopardy is The Joint Commission immediate threat to health and safety finding. Though rare, this is the most serious finding and exceeds the condition level finding. When surveyors see such a threat, they call headquarters in Chicago immediately and report what they have seen. If they get approval to designate this finding as an immediate threat, the surveyors go to the CEO of the hospital and say: “This needs to be corrected immediately or by the end of the day.”
Many immediate threat to health and safety findings relate to sterile processing or HLD and include the following:
IC.02.02.01, EP 2
• Not following manufacturer’s instructions for use (MIFU) for HLD and/or sterilization of equipment/instruments
• Reprocessing single-use instruments
• Evidence of oxidation on surgical/procedural instruments that would prevent sterilization.
• Improperly applied or deteriorated identification tape on sterile instruments
• Instrument identification tape being used contrary to MIFU.
HR.01.05.03, EP 1
• Lack of competency and training for staff performing HLD/sterilization/immediate use steam sterilization (IUSS)
• Staff performing IUSS unable to discuss appropriate sterilization parameters based on MIFU
• Frontline staff not aware when instruments are in disrepair and not safe for patient use.
IC.01.01.01, EP 4
• Not holding staff accountable related to high-risk processes or for compliance with MIFU when reprocessing instruments.
LD.04.01.07, EP 1
• Leadership oversight for reprocessing of instruments
• Leadership oversight for sterilization and HLD practices.
Some of these become double and triple findings; for example getting a finding for reprocessing single-use instruments will trigger a finding for HR competency. In other words, “somebody should have known not to do that,” says Rosing. It can also be a finding for infection prevention leadership, who should have been overseeing this in some way to prevent it from happening, he says.
Part of the problem with reusing single-use instruments has to do with COVID-19 supply chain problems. Organizations bought disposable instruments when they could not get reusable. Then because they look like they are reusable, they were put into inventory with the instruments approved for reprocessing. “This has been a big issue,” Rosing says.
To avoid this finding, Rosing recommends:
• Working with purchasing and any ancillary departments responsible for buying instruments in the past 12 months
• Reviewing purchase orders and MIFU to ensure instruments are approved for reprocessing
• Looking in inventory for single-use purchased items that have been mistakenly treated as reprocessable
• All hands on deck to find these in inventory
• Creating visual checklists for staffing, instruments, and integrity.
Surveyors will go through instruments looking for these single-use items.
Standards are dynamic
The Joint Commission is going to launch a new effort beginning in January 2023 to eliminate standards they believe are unnecessary or do not correlate to CMS CoP.
Also, beginning January 2023, they are adding some new and revised standards, such as those to reduce healthcare disparities:
• A new standard in the LD chapter has six new EPs that address healthcare disparities as a quality and safety priority.
• The Record of Care, Treatment, and Services requirement to collect patient race and ethnicity information has been revised.
• The Rights and Responsibilities of the Individual requirement prohibiting discrimination will apply to all Joint Commission accredited organizations.
In addition, The Joint Commission has added safety briefings to all accreditation surveys as well as certification and verification reviews, effective January 1, 2023.
The informal, 5-minute briefing allows organizations to tell surveyors and reviewers about any potential safety concerns and how they should respond if the safety plans are implemented while they are on-site. The briefing also will be incorporated into the first day of surveys or reviews.
Topics an organization should be prepared to discuss during the briefing are:
• Fire, smoke, or other emergencies
• Workplace violence, including active shooter scenarios
• Specific issues the surveyors or reviewers may encounter while on-site.
Revisions to the Sentinel Event Policy definition of a sexual abuse/assault event also became effective on January 1, 2023. The new definition addresses updates and aligns criteria for sexual assault events with external entities and provides clearer, more concise guidance when identifying such events and expectations. ORM
—Judith M. Mathias, MA, BS, RN, is the clinical editor of OR Manager and was clinical editor of the AORN Journal.
References
Rosing J. Mastering Joint Commission standards and CMS regulations. OR Manager Conference. 2022.
 Free Daily News
Free Daily News
- In-house 3D printing reduces hospital surgery times, costs
- North Korean hackers extort hospitals to fund attacks on US government
- ‘Best Medical School’ methodology updated for release of latest annual rankings
- Rural hospitals shutter labor, delivery units
- Less-invasive anesthesia technique improves pediatric surgery safety, patient experience
- Physician survey illuminates negative impact of prior authorization
- Volunteer surgeons publish eye-witness account of civilian carnage in Gaza
- HCA reports strong Q2 performance, sees decline in labor costs
- One expert concerned over drug shortages record high
- Trends in ASC industry as highlighted by one expert