OR Manager
Capitalizing on the New Wave of Hybrid ORs

About 100 US hospitals now have a hybrid operating room, and a 15% increase is projected over the next decade, according to experts who have managed installations at numerous facilities. Whether your hospital is considering converting a conventional operating room into a hybrid OR or building a brand new room, it’s important to know where you want to end up before you take the first step to get there.
“Knowing what you want to accomplish—having a business plan—is the most critical part of planning. Just knowing that you want to have a hybrid OR isn’t very helpful,”
- says Lynne Ingle, MHA, BS, RN, CNOR.
As a project manager with Gene Burton & Associates, a health care technology consulting company in Franklin, Tennessee, Ingle has overseen several hybrid OR installations. As a former director of surgical services, she is well versed in the kinds of improvements hospitals hope to achieve with the new technology.
Key players in the planning process are hospital administration, interventional cardiologists, open heart and vascular physicians, neurosurgeons, anesthesia providers, department heads and staff from the cardiac catheterization lab and the OR, a charge nurse, a staff nurse, and information technology, Ingle says. Participants from the nonclinical side include architects, vendors, and engineers. And for any remodeling project, it’s critical to consider infection prevention, she emphasizes. Start by determining just how your hospital defines “hybrid.”
The list of procedures that can be performed in a hybrid OR is growing. Among these are many cardiac procedures that in the past have been done in the cath lab, but Ingle notes that “hybrid ORs should not be glorified cath labs.” Newer procedures include transcatheter aortic valve replacement (TAVR) and mitral valve clipping, endoscopic abdominal aortic aneurysm, and aortic arch repair. Some hospital leaders have mistakenly believed that for a procedure such as an aortic valve replacement, a cath lab can be turned into a hybrid room, she says. However, some valve vendors won’t enter into a contract with a hospital if these procedures are to be performed outside the restricted area of the surgical suite. “You need to have all the capabilities for converting to an open procedure if need be,” Ingle says.
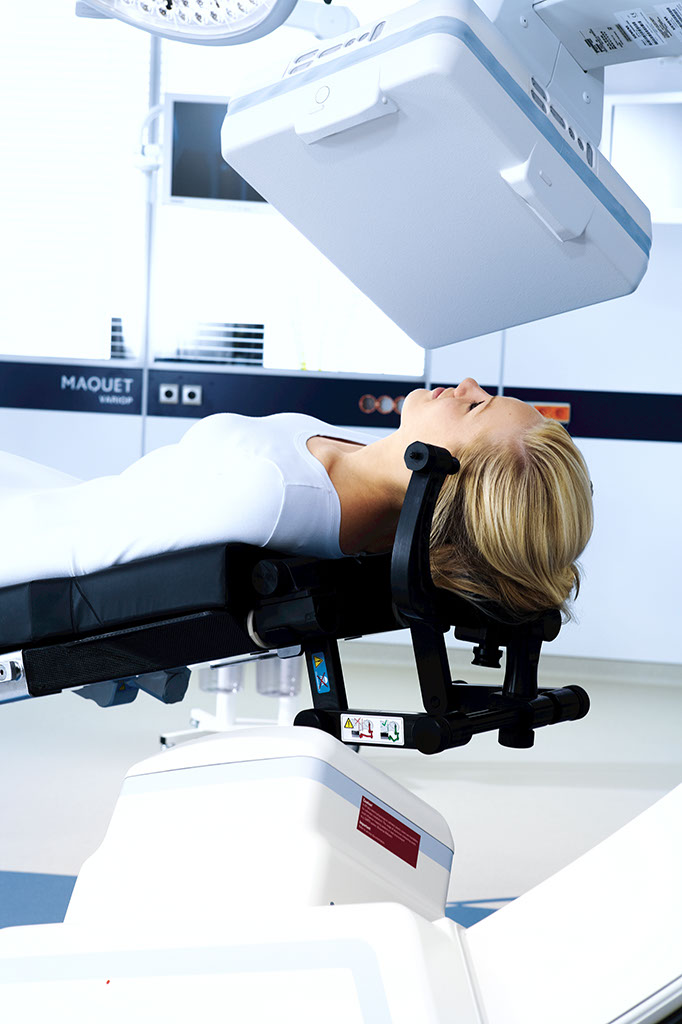
The most common configuration for a hybrid OR includes a single-plane angiographic x-ray imaging system and surgical equipment for open cardiac surgery.
Lights for the hybrid OR must have a longer arm reach, especially depending on who’s doing the imaging, Ingle says. Whether a ceiling-mounted or floor-mounted C-arm is the best choice depends on which procedures will be done in the room. Placement of lights and booms is important because anesthesia staff must be able to have access to the head of the table.
Knowing how the space will be used is especially important for determining the type of table that’s needed. If most procedures will be interventional, the table selected should be one that communicates with the imaging system, which is typically purchased from the imaging vendor. If the room will function primarily as an OR, the table selected should be appropriate for surgical procedures and integrated with the imaging system to allow for Image Guided Surgery. Some OR vendors offer a table with a fixed base and two tabletops—one for surgical procedures and one for imaging procedures.
Well-funded facilities may have a dedicated wall for imaging. But in general, facilities need to have a “live” monitor and a reference monitor from the imaging vendor, displays at the OR table for the surgeon and assistant, and displays on the wall—as few or as many as hospitals can afford or want, Ingle says.














Knowing the visuals needed in the control room is an important factor in deciding on vendors, she notes, because the technician in the control room must be able to see and understand what the surgeon needs.
As an example of the efficiency gain that’s achieved with a hybrid OR, Ingle says, troubleshooting can be done in one place instead of moving the patient from room to room. “For cardiac surgery, sometimes a patient is taken from the cath lab directly to the OR, and measurements are taken for vessels behind the heart, which can’t be seen. If the patient then moves to the ICU but isn’t doing well, the patient must go back to the cath lab for imaging and then back to the OR,” she says. “If everything were done in the hybrid OR, the surgeon would see the vessels right there because imaging would be done. That would cut down on morbidity, infection, and cost, and the patient could be discharged in a more timely manner.”
Hybrid ORs can also benefit patients in remote areas. Ingle was involved in a $3 million hybrid OR installation at St. Rose Dominican Hospital Siena Campus in Henderson, Nevada, in 2012.
“A multi-disciplinary ‘TAVR Heart Team,’ led by cardiothoracic surgeons and interventional cardiologists, has been through a comprehensive training program that includes procedure and complication management,” according to Rod Davis, president and CEO of St. Rose Dominican Hospitals and senior vice president of operations, Dignity Health Nevada. TAVR allows cardiac specialists to deliver and place a new aortic heart valve in the heart through a noninvasive procedure that doesn’t require cutting through the sternum or stopping the patient’s heart.
Previously, patients in that area of Nevada who were too ill to undergo aortic valve replacement with an open procedure usually had to go to southern California, Ingle says. Installation of the hybrid OR allowed them to have TAVR without having to travel.
"A hybrid OR lends itself to spinal surgery because it has real-time data with the C-arm and high-definition 3D pictures,"
‐ Elizabeth Wood
In 2013, the interventional trauma operating room (ITOR)—a $6-million 1,600-square-foot hybrid operating suite—opened at the Foothills Medical Center in Calgary, Alberta, Canada. The facility is “the first of its kind designed specifically for trauma patients [and] is more than twice the size of a traditional OR,” according to Andrew Kirkpatrick, MD, Alberta Health Services’ medical director of trauma services. The angiography equipment, which allows surgical and diagnostic imaging teams to work on patients at the same time, makes it possible for patients with severe bleeding to go directly to the ITOR for treatment. Whether future hybrid ORs in the US will be built specifically for trauma patients remains to be seen, but Ingle says it’s a good bet that more spinal procedures will be done in hybrid ORs of the future.
“A hybrid OR lends itself to spinal surgery because it has real-time data with the C-arm and high-definition 3D pictures,” she explains. “You can’t see those as well with a mobile C-arm that must be rolled into the room. The hybrid room equipment allows the surgeon to see on the screen where to place surgical components like screws and plates.” While most hybrid ORs initially were installed in university hospitals, an increasing number of community hospitals have added or are planning to add at least one hybrid OR, Ingle says.
You’ve cleared the hurdle of installing a new hybrid operating room, but now another hurdle looms: putting it into operation.
The good news is you likely have already built a collaborative relationship among key players. “Getting everyone on the same page to justify the OR sets the team up for success,” says T. Brett Reece, MD, a faculty member in the division of cardiothoracic surgery for the University of Colorado Hospital (UCH) in Aurora, which opened its hybrid OR in April 2012. About 30 to 40 cases, mostly endovascular, are done each month, with utilization between 66% to 80% during weekday business hours. You’ll need to build on that collaboration in four areas: education, staffing, supplies/billing, and coordination.
“We used multiple opportunities to educate staff,” says Tamara Mayne, BSN, RN, cardiothoracic surgery service specialist for the UCH OR. “The educators in interventional services and the OR partnered because they had the knowledge of how it would function and what information staff needed.”
The hybrid OR was open for a full week before the first case, giving staff and physicians time for training and learning about the equipment, which includes fluoroscopy imaging, a surgical table, equipment booms, and general imaging. Everyone on the OR staff was oriented to the hybrid OR to provide flexibility, although the vascular team members work there most frequently.
Education included how to set up the room. “We adapted current space to the hybrid OR, so we had to fit everything in so that it would work,” Mayne says. That attention to detail is important for a successful case. For example, she adds, “If you don’t move the C-arm correctly, you can’t move the lights.”
Physician preference added to the complexity. “You have to have a way to set up every room for every case for every physician,” says Dr Reece. Mayne turned to the traditional preference card as a tool, but with a twist. “We have lots of pictures and 3-D drawings showing how everything needs to be positioned,” she says. Mayne keeps the images on her office computer. Education helped ease what Dr Reece feels was the most challenging part of the startup—anxiety among those in the room. “The consistency that Tamara provided made it work,” he says. “We overcame anxiety through repetition in education and leading by example,” Mayne adds. “Now anxiety is low. People have a good idea of how to fit everything in the room and how the process works.”
“We use a blended staffing model for the hybrid OR,” says Katherine Halverson-Carpenter, MBA, RN, CNOR, patient care services director for obstetrics and perioperative series at UHC. Staffing is based on case type. Staff from the cardiovascular (CV) center and the OR handle combined cardiology and surgical procedures, with the CV center nurses supporting the cardiologists with imaging and documentation. A radiology technician from the interventional radiology (IR) department fills that role for IR procedures done in the hybrid OR. One challenge has been the finite number of radiology technicians with the skill set to work in the hybrid OR, Halverson-Carpenter says.
Supply and billing needs “Managing supplies is a challenge,” says Mayne. Vascular surgeons (some of whom were new to UCH), interventional radiologists, and interventional cardiologists had to feel confident that the supplies they needed would be available, while OR leaders needed to reduce redundancy as much as possible.
The OR is working on obtaining high-volume supplies on consignment to avoid replicating supplies in the IR and CV center suites. Billing processes also had to be established. The IR department and CV center bill by the procedure, but the OR bills by time. “We got the finance team together and decided we would bill by the minute because the procedure was done in the OR,” says Halverson-Carpenter. If the procedure is done in interventional radiology or the CV center, billing is done by procedure.
“The greatest challenge of a hybrid OR is the coordination,” says Halverson-Carpenter. At UCH a hybrid steering committee provides oversight and helps work through problems. Halverson-Carpenter and Dr Reece, who allocate the block time, cochair the committee. Among members are those who perform procedures in the room, nursing staff, nurse managers, and perioperative business managers from the IR department, OR, and CV center.
Halverson-Carpenter says the committee reviews utilization of the room both during regular business hours and after hours, which cases are being done by which physicians, supply needs, billing, and any operational issues. “It’s important to track your volume and who is using the room so you can readjust your block time allocation,” she notes.
One discussion centered on the use of the hybrid OR for traditional surgical procedures. Recently UCH opened four new ORs; once they are fully staffed, the hybrid OR will be dedicated to hybrid cases.
Halverson-Carpenter credits the success of the committee and the hybrid OR to a meeting she and the chair of surgery cochaired early in the planning process.
The meeting focused on the principles of collaboration and included key stakeholders, such as the medical director of IR, section head of vascular surgery, chair of cardiothoracic surgery, chair of cardiology, all physicians and surgeons who would be working in the room, and administrators for the OR and CV center. “Establishing the framework clarified our mutual goals and purpose,” Halverson-Carpenter says. “It became an expectation that people would collaborate.” The group met with the vendors, conducted site visits, and worked with designers during the process.
That spirit of collaboration carried over into operations meetings among centers, where details were hammered out. The team had to consider current practices while determining how to best work together, something they continue to do. “We respect the practices and philosophies of each of the individual units,” Halverson-Carpenter says. “That’s helped us come together as a team.”
Staff, physicians, and patients are satisfied with the hybrid OR at UCH. “We are able to do cases now that we weren’t able to do safely previously,” says Dr Reece. Those include fenestrated grafts for patients with complex anatomy and percutaneous cardiac valves. “We can reinvent what we provide to patients.” “Everyone working together has made the program successful,” adds Mayne. “We’ve been a tight-knit group.” That success is expected to pay off; the UCH team is in the process of justifying a second hybrid OR.”
"Everyone working together has made the program successful," adds Mayne. "We've been a tight-knit group."
- Tamara Mayne, BSN, RN


Endovascular hybrid operating rooms are no longer limited to university medical centers, as community hospitals expand their cardiovascular services. According to Dorothy Urschel, MS, MBA, RNFA, ACNP-C, NEA-BC, three main trends are stimulating the growth of hybrid ORs: “Cardiac surgery is becoming less invasive, interventional cardiology is becoming more invasive, and vascular surgery continues to be minimally invasive and use catheter techniques combined with radiology techniques.”
Urschel is cardiac and vascular service line director at St Peter’s Health Partners, a system of four community hospitals in Albany, New York. ECRI Institute, which assists hospitals with strategic planning and technology assessment, has seen about a 10% annual growth in requests related to hybrid ORs among its 3,500 hospital members. The trend of more hybrid ORs—including those in community hospitals—is likely to continue. But a successful hybrid program requires careful analysis and planning by a multidisciplinary team. “Start with the patient, and work your way back to determine what you need,” says Thomas Skorup, MBA, FACHE, vice president of applied solutions for ECRI Institute. “Technology supports practice, it doesn’t drive it.”
 Emergence of True Hybrid Cardiovascular Procedures
Emergence of True Hybrid Cardiovascular Procedures
 Technical Advancement Requiring Sterile Space
Technical Advancement Requiring Sterile Space

In its report “Hybrid Operating Rooms with a Focus on Endovascular Hybrid ORs,” ECRI Institute says hybrid ORs are a good fit for high-risk, minimally invasive cardiovascular procedures that require advanced imaging and may require transition to open surgery.
Skorup, who says that “advanced imaging” typically refers to an angiography system‐ as opposed to CT or MRI‐ points to approval of the Sapien (Edwards Lifesciences) transcatheter aortic valve in 2011 as a major stimulus for endovascular hybrid ORs. Transcatheter aortic valve replacement (TAVR) “exemplifies what a hybrid OR is all about,” he says. “It’s not a traditional vascular intervention. We’re not performing an open procedure or reinforcing a vessel with a stent; we’re replacing a surgical procedure by performing a procedure through a catheter.” Before TAVR, nearly a third of patients with severe aortic disease weren’t candidates for surgery, so adding this new procedure has expanded the market‐ and saved lives. “One randomized, controlled trial showed that TAVR significantly reduced mortality rates at 1 year and at 2 years,” Skorup says.
Other procedures typically performed in an endovascular hybrid OR include combination coronary artery bypass graft (CABG)/percutaneous coronary intervention (PCI) and endovascular aneurysm repair. At St Peter’s Health Partners, physicians perform a wide range of procedures, including stent graft placement and various types of aortic surgery.
“It’s amazing what you can do,” says Urschel. “We have doubled the number of procedures we anticipated when we were in the planning stage.” Block time is 75% efficient. Although their hybrid room is not exclusively for endovascular procedures, most cases are vascular. Urschel notes a number of factors have contributed to the program’s success, starting with multidisciplinary planning.
St Peter’s created a hybrid OR steering committee composed of key players, including vascular and cardiovascular surgeons, cardiologists, OR nursing leaders, and supply chain managers. “You need to have physician buy in by having them at the table,” Urschel notes.
Becky Chalupa, MS, RN, CNOR, associate chief nursing officer at Methodist Sugar Land Hospital in Texas, adds that other needed players are anesthesia and facility managers. Methodist has 243 beds, 18 ORs, and one endovascular hybrid OR that opened in December 2012.
“Each hospital has a different case mix,” Skorup says. “You need to take a surgical time-out to define the case mix you expect and use that as a template for your planning efforts. You then have a greater likelihood of engaging the right people and having success.” He recommends considering all options. “If you plan for only one specialty, you have limited the future of the room and may not have the volume you need to be successful,” he says.
“Hospitals don’t have money to lose.” For example, Urschel says, St Peter’s had a second OR fitted for hybrid capability at the same time as the first. “Then we can just add the robotic C-arm when we have sufficient volume to justify its purchase.”
Urschel says the steering committee developed a list of procedures to be performed in the hybrid OR, which helped smooth some of the later bumps in the road when it came to scheduling block time.
All this equipment means that hybrid ORs are typically about 500 sq.ft. larger than traditional ORs.
People who need to be part of the planning process, but are sometimes forgotten, include perfusionists and radiology technicians, according to Skorup. “Having a surgeon working with an angiographic technician in the OR is a new working environment,” he says. “You have to determine how the procedure will flow.” Of course, building management is also key, whether constructing a new OR or retrofitting an old OR for hybrid capability. For example, the floor has to be of sufficient strength to support the weight of the equipment, the ceiling support must be sufficient for hanging booms, and the room needs walls that provide radiation protection. Skorup adds that the choice of floor versus ceiling mount ultimately comes down to physician preference.
As with most projects, planning takes time. Urschel says planning started 3 years before the OR opened. And, senior management will want a detailed business plan showing return on investment, especially since hybrid ORs aren’t cheap. Urschel says if no rebuilding is necessary, you’ll still need to plan on more than $3.5 million for the basic equipment.
To choose equipment vendors, Skorup says you should “define what you want to accomplish, define your needs, and then determine which vendor fits those needs.” A common mistake is to allow a vendor to have early discussions with a single person who then becomes an advocate for a particular system and is not open to other options. Urschel adds that visiting other facilities with hybrid ORs helps identify what works and what doesn’t.
The hospital is now looking at options for changing equipment, but construction will be needed. Skorup says that standardization is difficult at this stage because system configurations aren’t “mature,” as is the case with CT scanners. However, that may change in the future.
Skorup notes that many ORs forget to give the supply chain the attention it requires. “Representatives from the supply chain need to be involved early,” he says. A top consideration is determining what will be stocked in the interventional cardiology lab and what will be stocked in the hybrid OR. “Consider the cost of replicating cath lab supply in the OR,” he notes. “But not replicating supplies can lengthen OR procedure time when personnel have to wait on supplies being obtained from the cath lab.” Urschel agrees with the importance of supply chain management. The team ultimately decided to keep vascular wires on a cart that the interventional cardiology lab and OR can share.
One of the biggest challenges for a hybrid OR is managing personnel. Depending on the procedure, those in the room might include the anesthesiologist and anesthesia technician, vascular and cardiothoracic surgeons, interventional cardiologist physician assistant, scrub technician, circulator, interventional cardiology technician, and radiology technician. “It’s combining a cath lab and an OR team,” says Urschel, who notes she needed to add 4.2 full-time equivalent (FTE) employees to open the room. Cross training between the OR and the interventional cardiology lab is essential and requires good management skills. “They have to learn how to work with a different team, so you have to explain how each team works,” says Urschel. “You need to work with the team very closely.” She adds that training staff in “radiation hygiene” should be a key component. Chalupa says Methodist has a core team for the hybrid room. Two backup radiology technicians are available on the day shift, and there is an evening technician who is trained for the hybrid OR. The technicians take call.
To educate staff, Chalupa had a radiology technician attend training provided by the manufacturer, and both radiology technicians and nurses spent time in hybrid ORs in other hospitals within the Methodist system. Chalupa held three dry runs before the first case. The dry runs turned up problems: Neither the equipment needed to perform bolus chasing nor the intercom system had been installed as requested. The dry runs also helped determine the room setup, which Chalupa says varies according to type of case as well as physician and anesthesia preferences.



Skorup notes that data show a “strong correlation between a recommended number of procedures and maintaining competence” for surgical robotics teams, and he expects that to extend to transcatheter procedures such as TAVR. It’s important to have a plan for determining staff and physician competence in the procedures being performed. In some cases, guidelines are available. For example, the Centers for Medicare and Medicaid Services outlines requirements that must be met to obtain reimbursement for TAVR. These include specific volume guidelines for the cardiovascular surgeon and the interventional cardiologist.
On the horizon
Before looking ahead, Urschel recommends looking back. “Conduct a financial and operational analysis 1 year after you open the OR to see where you are,” she says. For example, the analysis at St Peter’s resulted in staffing adjustments. In the future, the use of hybrid ORs is likely to continue expanding. Skorup expects to see more multiple interventions for individual patients. “Some centers are doing vessel verification after a CABG procedure,” he says. He adds that physicians in Europe are performing transcatheter mitral valve repair, and he expects the procedure to emerge in 2 to 3 years.
—Cynthia Saver, MS, RN
Maquet offers the most complete portfolio of any supplier in a Hybrid OR. As part of our commitment to our customers, we offer planning, design, installation and surgical equipment expertise to help you build a room that’s ideal for your needs and budget – while ensuring that you’re capitalizing on every cost efficiency and savings opportunity along the way.
For more information about Hybrid OR or its components, please contact David Browne at [email protected] or 973-709-7202.
Hybrid ORs are proliferating in response to market, surgeon, and even patient demands, but building the business case for this technology can be challenging.
“It’s a very expensive proposition,” says Lynne Ingle, MHA, BS, RN, CNOR, project manager for Gene Burton & Associates, a healthcare technology consulting company in Franklin, Tennessee, and a former director of surgical services. Costs can average from $3 million to $6 million, according to data from ECRI Institute and The Advisory Board Company.
With that much money at stake, the natural first question is, “Does our hospital need a hybrid OR?” When answering this question, OR managers should keep in mind that a hybrid OR is a long-term investment; short-term profits are unlikely.
Staying competitive
“I think we’re at the point that you need a hybrid OR to be competitive,” says Deborah Rideout, BSN, RN, CNOR, director of perioperative services at Southcoast Hospitals Group in New Bedford, Massachusetts. The first hybrid OR in this four-facility system opened in New Bedford in 2008, and another one is being built at their Fall River site. About 230 cases per year on average are performed at the New Bedford site.
Rohit Inamdar, senior medical physicist at ECRI Institute, agrees with Rideout. “Even if you are a small facility, minimally invasive surgery is here to stay, so if you don’t get on board with a hybrid OR or cath lab, you will be left behind,” says Inamdar, who has consulted with many hospitals developing hybrid rooms. “You need a hybrid OR to keep your cardiac surgery program.”
Although academic medical centers remain the most common site, Inamdar has seen a growing number of hybrid ORs being installed in community hospitals.
If hybrid ORs are a growing trend, how can OR managers build a business case that provides a reasonable return on investment? Inamdar says program, staffing, and patients form a three-legged stool that supports the business case for a hybrid OR.
"I think we're at the point that you need a hybrid OR to be competitive,"
Deborah Rideout, BSN, RN, CNOR
Director of Perioperative Services at Southcoast Hospitals Group in New Bedford, Massachusetts
Inamdar recommends that anyone considering a hybrid OR first determine if the facility has a robust open-heart surgery program for valve replacement, given that currently the primary procedures performed in the hybrid OR are transcatheter aortic and mitral valve replacement (TAVR, TMVR).
OR managers should also consider other potential future uses of the hybrid OR. At Inova Fairfax in Falls Church, Virginia, for example, the endovascular hybrid OR began as a location for TAVR, but has since expanded to include endovascular aneurysm repair, says Anne Cochrane, MSN, RN, CNOR, interim director of the cardiovascular OR. “You want to set up the room so it can be used for anticipated future procedures,” she says.
Planned future use also affects design and equipment needs. For instance, Ingle says, “Some neuro-surgeons want a biplane [angiograph imaging system], but endovascular surgeons use a single plane, and some neurosurgeons are OK with a single plane and don’t need a biplane.” These decisions will affect costs.
The geographic location of the hybrid room affects the bottom line. “CMS [Centers for Medicare & Medicaid Services] says you have to do TAVR in a hybrid room to receive reimbursement,” Inamdar says. CMS lists additional qualifications needed for reimbursement, including volume requirements. Third-party payers are also providing incremental reimbursement for TAVR. In 2014, CMS approved a technology add-on payment to cover TAVR.
To support the hybrid OR, the program must be supported by a good relationship with primary care physicians who will refer patients. “If you have good vascular surgeons but don’t have any primary care alliance, you could find yourself with an empty room,” Rideout says. “You have to have strong primary care alliances.”
Writing a business plan isn’t done in isolation, says Deborah Rideout, BSN, RN, CNOR, director of perioperative services at Southcoast Hospitals Group in New Bedford, Massachusetts. “It takes a team to collect the information you need and put it into one packet.”
The team should include surgeons, and staff from business, finance, engineering, imaging, and biomedical, among others. Typically the plan projects breaking even at 5 years.
“Sales reps can be helpful in identifying break-even points,” says Anne Cochrane, MSN, RN, CNOR, interim director of the cardiovascular OR at Inova Fairfax in Falls Church, Virginia.
“You should have cardiac surgeons who have experience and expertise with TAVR because these patients are considered high risk,” Inamdar says.
For hospitals without TAVR experience, CMS requires cardiovascular surgeons to have performed at least 100 career aortic valve replacements (AVRs), including 10 high-risk patients, or at least 25 AVRs in 1 year, or at least 50 AVRs in 2 years, which include at least 20 AVRs in the last year before TAVR initiation. Hospitals may need to recruit cardiovascular surgeons or interventional cardiologists to meet these numbers.
Surgeons need to maintain volume to ensure continued reimbursement. CMS requires the surgeon and hospital to complete at least 20 TAVR procedures in a year, or at least 40 TAVR procedures in 2 years. The agency also has volume requirements for interventional cardiologists and the hospital’s cardiac catheterization lab. For example, the cath lab must perform at least 1,000 catheterizations per year, including at least 400 percutaneous coronary interventions per year.
In addition to physicians, CMS lists other members who must be part of the team, including echocardiographers, imaging specialists, heart failure specialists, cardiac anesthesiologists, intensivists, nurses, and social workers.
Above all, says Ingle, “The most critical part is having physician champion.”
To analyze potential patient volume, Rideout suggests asking, "What is the market share that we aren't getting because we don't have a hybrid OR?" It's helpful to list cases that will be done immediately in the hybrid OR and those that will be added later.
"Look at the length of stay for those patients, and work with your business partners in the organization to calculate what the savings would be if those patients could be discharged sooner," she adds.
Cochrane, who has several years of OR experience in a variety of OR settings, says the surgeons are good predictors of volume. "They really know their market and where their referral base is," she says, adding, "It's better to underanticipate than overanticipate the numbers."
Because a limited number of procedures currently require a hybrid OR, hospitials can run into financial difficulties. "There can be a positive profit margin with TAVR, but it's very small," Inamdar says, noting that many facilities may struggle to break even.
Part of the difficulty is that only a small number of patients are currently eligible for the procedure, and those who are eligible are also high risk. "The national TAVR is about 20,000 to 30,000 in the entire US," Inamdar notes.
Reimbursement for the procedure from CMS ranges from $27,000 to $56,000, depending on the patient's severity and how he or she is treated. Considering that the TAVR valve costs just over $30,000 and that the procedure cost ranges from $50,000 to $80,000, it's clear that a hybrid OR "is not a money-making machine," Inamdar says.
"If you're armed with talented physicians who are aligned with you, have a solid cardiovascular program, and a market share that is validated to be leaving the area because you're not offering certain services--that's a good case for a hybrid OR," says Rideout.
Because of the expense, it’s not easy to make the numbers work for a hybrid OR. “But because it [a hybrid OR] has become a standard, you have to find ways of being fiscally prudent while you’re doing it,” Rideout says.
One way of saving money is to choose vendors wisely, Ingle says. If, for instance, the cath lab is already using equipment from Toshiba, the OR manager might be able to obtain a discount by purchasing Toshiba equipment for the hybrid OR. “You will have multiple vendors, so coordination is really important,” she adds.
If your cardiac surgery program isn’t large enough for a hybrid OR, Inamdar suggests considering a hybrid cath lab or adding a hybrid interventional radiology (IR) suite.
The downside is that these rooms still require the staff, supplies, and sterility needed in the OR. “But it’s doable and it’s a lower price option,” Inamdar says.
Ingle adds, “My philosophy is that it should be behind the red line of the OR in case you have to open the patient, but I’ve seen it done both ways. It’s something hospitals have to discuss.” She notes that remodeling an existing OR is less expensive than building a new one.
To maximize the use of the hybrid OR, Inamdar recommends OR managers work with other physicians such as vascular surgeons, neurosurgeons, and electrophysiologists, who use angiography imaging systems. “You might be able to consolidate so you need fewer labs, and improve your financial equation a bit,” Inamdar says.
Keep in mind that when not in use for its hybrid capabilities, the OR can be used for certain other cases. At Inova, for instance, “the hybrid OR is built so it can be used for any patient who requires a bypass pump,” Cochrane says.
Ingle reports that hybrid OR use is being expanded at many hospitals to include spinal and total joint replacement surgery, as well as other cardiovascular procedures, as physicians increasingly tap into the value of good imaging for a variety of procedures.
Another option for reducing costs is to choose a refurbished angiography imaging system. Facilities that are downsizing or upgrading their systems may be trading in systems that are less than 5 years old.
Inamdar says the typical life span of these systems is 10 years, so facilities could save as much as $1 million by purchasing a refurbished model. “It will still meet your needs but won’t have all the bells and whistles,” he says. When exploring the refurbished option, be sure to work with a reputable vendor.
"But because it [a hybrid OR] has become a standard, you have to find ways of being fiscally prudent while you're doing it,"
Deborah Rideout, BSN, RN, CNOR
Director of Perioperative Services at Southcoast Hospitals Group in New Bedford, Massachusetts
Inamdar notes that currently only one mitral valve contouring system is approved for use in the United States, but expects others currently being used in Europe to receive approval as well, further pushing demand for hybrid ORs. “Transcatheter devices are a growth area, and I don’t see it slowing down anytime soon,” he says.
Presented By
Design, Layout, and Interaction: The Digital Development Team @ AI
Copyright © 2015 Access Intelligence, LLC.
{kind=link}
{kind=link}
{kind=link}
{kind=link}